A pathological demand avoidance test isn’t something you can just take, like a blood test or a brain scan. It's not a single, clear-cut procedure. Instead, it’s a name for the in-depth evaluation process clinicians use to identify a specific profile of behaviors, most often seen within the autism spectrum.
This profile is defined by an intense, anxiety-driven need to avoid everyday demands.
What a Pathological Demand Avoidance Test Actually Is

When you hear the word “test,” it’s easy to picture a standardized assessment with a clear pass or fail. But identifying a Pathological Demand Avoidance (PDA) profile is much more like putting together a diagnostic puzzle than taking a quiz. It’s an investigative process that brings together multiple sources of information to paint a complete picture of an individual's unique way of being.
Think of it less like a single exam and more like a detailed case study. A skilled clinician is like a detective, gathering clues from different places to understand not just what a person does, but why they do it. This is a critical distinction because the motivation behind the behavior is what truly separates PDA from other conditions.
The Foundation of PDA Understanding
The journey to understand PDA started back in the 1980s. Professor Elizabeth Newson first noticed a distinct group of autistic children who showed an obsessive resistance to everyday demands. This wasn't simple defiance or a behavioral choice; it was a deeply ingrained, anxiety-fueled response.
Since then, research has confirmed that PDA traits aren't all that uncommon within the autistic community. One study found that among a sample of autistic individuals, nearly 25% showed some to substantial PDA features. This context helps explain why a simple checklist just won’t cut it. The assessment has to dig deeper.
At its core, a PDA assessment seeks to understand the "why" behind the avoidance. Is it a refusal to follow rules, or is it an instinctive, anxiety-driven need to maintain control and autonomy in the face of overwhelming pressure?
Components of a Comprehensive Evaluation
Because there’s no single, official "pathological demand avoidance test," clinicians rely on a multi-faceted approach. This process is absolutely essential for telling PDA apart from other presentations and making sure the right support strategies are put in place.
Here are the key components:
- Clinical Interviews: These are in-depth conversations with the individual (if they’re old enough) and their family. The goal is to gather a detailed developmental history and get a real sense of their current challenges.
- Behavioral Observation: Watching how someone interacts in different settings—either in person or through telehealth—provides invaluable insights. It shows a clinician their social strategies and how they respond to demands in real-time.
- Screening Questionnaires: Tools like the Extreme Demand Avoidance Questionnaire (EDA-Q) can help identify and quantify specific traits linked to the PDA profile.
- Collateral Information: Getting feedback from teachers, other therapists, and professionals who know the person well helps create a 360-degree view of how they function across different environments.
This thorough process ensures that a potential PDA profile is looked at within the full context of a person’s life. Understanding this is often the first step toward seeking the right kind of evaluation, like a specialized autism screening for adults that can explore these more nuanced presentations.
Using Screening Tools Like the EDA-Q
When families or educators first suspect a Pathological Demand Avoidance profile, they often look for some way to get initial clarity. That's where screening tools come in.
It's important to be clear: these are not a formal pathological demand avoidance test. They're questionnaires designed to highlight specific traits. Think of them as a compass pointing you in a potential direction, not the final destination.
The most well-known of these is the Extreme Demand Avoidance Questionnaire (EDA-Q). It was created to help parents and teachers systematically report on behaviors they observe. It’s a way of organizing those often-chaotic observations into a structured format that can be incredibly useful when you eventually speak with a clinician.
There's also a shorter, more streamlined version called the EDA-8. This eight-question screener is designed for quick identification of key PDA traits, making it an accessible first step for many.
What Do These Screeners Actually Measure?
These questionnaires go far beyond simple defiance. They dig into the specific, nuanced behaviors that characterize the PDA profile, carefully crafted to identify patterns related to the anxiety-driven need to avoid demands. That anxiety piece is the key differentiator.
For example, the EDA-Q explores several core areas:
- Resistance to Ordinary Demands: Does the person resist simple, everyday requests that most others would comply with easily, like getting dressed or brushing their teeth?
- Use of Social Strategies: Does the individual use social tactics—like making excuses, creating a distraction, or using charm—to get out of doing things?
- Sudden Mood Changes: Is there a tendency for rapid shifts in mood, especially when a demand is placed on them? They may appear "socially labile."
- Comfort in Role Play: It also measures a person's comfort with fantasy or taking on different personas, which can be a sophisticated coping mechanism for avoiding demands.
These tools provide a structured way to quantify behaviors that can otherwise feel confusing and hard to explain. They give parents and professionals a common language to discuss what they're seeing.
Think of a PDA screener like a weather forecast. A forecast can tell you there's a 90% chance of a thunderstorm, giving you valuable information to prepare. However, it doesn't guarantee the storm will hit your house specifically. Similarly, a high score on the EDA-Q strongly suggests PDA traits but isn't a substitute for a full clinical evaluation.
For those interested in how different self-report measures are used, you can explore tools like the Autism Spectrum Quotient to see how various questionnaires contribute to a larger diagnostic picture.
Comparison of PDA Screening Questionnaires
To help clarify the differences between the two main screeners, here is a quick comparison.
| Feature | Extreme Demand Avoidance Questionnaire (EDA-Q) | Extreme Demand Avoidance-8 (EDA-8) |
|---|---|---|
| Purpose | Comprehensive screening for PDA traits | Quick, initial identification of key PDA traits |
| Length | 26 items | 8 items |
| Completed By | Parents or teachers | Parents or teachers |
| Measures | In-depth look at social strategies, mood lability, resistance, and role-play | Core features of demand avoidance |
Both tools serve a valuable purpose in the journey toward understanding. The EDA-8 is a great starting point, while the EDA-Q offers a more detailed picture that can be very helpful for a clinical team.
Interpreting the Results of a PDA Screener
So, you've completed a screener. What now? The results offer a preliminary sketch, not a definitive portrait. A high score is a significant indicator that a more formal investigation is a good idea. It’s the first piece of the puzzle.
Screeners are designed to capture the core features of a PDA profile that a clinician would explore in-depth. They help build a case for a deeper dive during a formal assessment, providing the initial data points that guide the clinical interview and observation process. This ensures that a professional evaluation can be focused and thorough from the very beginning.
The Tricky Landscape of PDA Assessment
If you're looking for a straightforward pathological demand avoidance test, you'll quickly find that it's not quite that simple. One of the biggest hurdles is that PDA is not currently a distinct diagnosis in the major diagnostic manuals professionals use, like the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders) or the ICD-11 (International Classification of Diseases).
This creates a real challenge. Without an official diagnostic code, getting a formal identification depends almost entirely on a clinician's personal expertise and how familiar they are with the PDA profile. It’s not something you can just check off a list; it’s a conclusion reached through deep clinical judgment.
It’s a bit like trying to describe the color teal to someone who only knows the words "blue" and "green." You have to explain it by combining concepts—"it's like blue, but with a hint of green"—because there's no single, official word for it in their vocabulary. This is what clinicians often have to do, describing PDA within the existing framework of autism.
Why Isn't There a Standardized Test?
The main reason you won't find a single, standardized test for PDA is that there's no universally agreed-upon clinical definition. While screeners like the EDA-Q are helpful for gathering information, they aren't diagnostic tools. They’re designed to flag traits, not to confirm a condition.
This lack of a standard has a domino effect. It makes it tough for researchers to conduct large-scale studies, which in turn means fewer professionals get trained to recognize the profile.
The real challenge is that PDA is all about the why behind a person's behavior—the anxiety-driven need to avoid demands—not just the what. A standardized test would have a hard time capturing that kind of nuanced, internal motivation.
What this means for families is that the quality of an assessment is directly tied to the experience of the person conducting it. Finding a professional who truly gets the subtle differences between PDA, ODD, and other autism presentations is absolutely key to getting an accurate and helpful evaluation.
Why Clinical Definitions Can Vary
Since PDA isn't in the DSM-5, clinicians don't have a single, official set of criteria they must follow. Instead, they work from a collection of characteristic traits first described by Elizabeth Newson and later built upon by organizations like the PDA Society and other experts.
This variability means one clinician might zero in on the use of social strategies to avoid demands, while another might focus more on the sudden mood swings or the intense need for control. Neither approach is necessarily wrong, but this inconsistency can lead to different conclusions from different professionals.
This has a direct impact on research and understanding how many people have PDA. The working definitions can vary so much that some studies find PDA to be rare, while others suggest it's relatively common. This gap makes it difficult to get a clear picture of PDA on a global scale. You can discover more insights about these prevalence challenges and the ongoing work to create a more consistent definition.
The Role and Limits of Screeners
Screening questionnaires are valuable, but it’s crucial to know what they can and can’t do.
- They Are Not Diagnostic: A high score on a screener like the EDA-Q is a strong sign that PDA traits are present, but it can't—and shouldn't—be used as a diagnosis on its own.
- They Rely on Observation: The accuracy of a screener depends on how the observer interprets behavior, which can be subjective. What one person sees as defiant, another might see as anxious.
- They Don’t Capture the Full Story: A questionnaire can't explain the environmental triggers or the internal state of anxiety that leads to demand avoidance.
Think of these tools as a starting point. They help you organize your observations and have a more productive conversation with a qualified professional. They provide the initial "clues" that a skilled clinical "detective" will use to build a complete picture during a full evaluation. Understanding these challenges from the outset helps you go into the assessment process with realistic expectations and the knowledge you need to advocate for a thorough, nuanced evaluation.
How Clinicians Tell the Difference Between PDA, ODD, and Autism
From a clinician's standpoint, teasing apart the behaviors of Pathological Demand Avoidance (PDA), Oppositional Defiant Disorder (ODD), and a more classic autism presentation is like a piece of diagnostic detective work. On the surface, they can look almost identical. It might be a child refusing school, an adult chronically avoiding work tasks, or sudden, intense emotional outbursts. A seasoned clinician knows the real clue isn't just what the person is doing, but digging deep to find out why.
This distinction is absolutely critical. The motivation driving the behavior completely changes which support strategies will be effective. In fact, an approach that works for a child with ODD could be the exact opposite of what a child with a PDA profile needs. That’s why a thorough assessment has to go beyond surface-level behavior to understand what’s happening on the inside.
The Core Motivational Difference
The central piece of this diagnostic puzzle is the root cause of the demand avoidance. While the action might be a simple "no," the internal experience behind that "no" is worlds apart for each profile.
Let's take a simple, everyday request: "It's time to put your shoes on."
- An individual with an ODD profile might refuse as a direct challenge to authority. The motivation is often external and rooted in a power struggle with the person making the request. It’s less about the shoes and more about defying who’s in charge.
- Someone with a classic autism profile might resist for a number of other reasons. Maybe the shoes feel wrong from a sensory perspective, or leaving the house right now disrupts a cherished routine. It could also be the jarring nature of transitioning from one activity to another. Here, the motivation is typically internal—an attempt to manage their sensory world and need for predictability.
- A person with a PDA profile resists because the request itself creates an immediate, overwhelming feeling of pressure. This pressure threatens their sense of autonomy, and the avoidance is an automatic, anxiety-driven reflex to escape that feeling of being controlled. It's not about the shoes, and it's not even really about the person asking. It's about the demand itself.
At its heart, the clinical differentiation comes down to a single question: Is the avoidance driven by a desire to defy authority, a need for predictability and sensory comfort, or an overwhelming, anxiety-fueled compulsion to escape demands and maintain control?
This fundamental difference is precisely what clinicians are searching for during a comprehensive evaluation—something that goes far deeper than a basic pathological demand avoidance test or questionnaire.
Looking at Social and Behavioral Patterns
Beyond that core motivation, clinicians start piecing together other clues from social interaction styles, behavioral patterns, and the person’s developmental history.
One of the key markers for a PDA profile is the use of surprisingly sophisticated social strategies to get out of demands. This can look like using charm, cracking jokes, making up elaborate excuses, or creating a clever distraction. This often stands in contrast to ODD, where defiance tends to be more direct and confrontational. It also differs from other autistic profiles where social communication challenges might make these kinds of social maneuvers less likely.
Another area clinicians look at is how the individual responds to things like structure and praise.
- Structure: While many autistic individuals find great comfort in predictable routines, someone with a PDA profile may resist those same structures because they feel like an imposed demand.
- Praise: Direct praise can actually ramp up anxiety for a PDAer. It can feel like a new demand to perform that same behavior again in the future. This is quite different from ODD, where praise might be met with neutrality or suspicion, and from other autistic profiles where it's often genuinely appreciated.
When trying to separate these traits, clinicians often map out the key differences in motivation and behavior.
Differentiating PDA vs ODD vs Classic Autism Traits
| Behavioral Trait | Pathological Demand Avoidance (PDA) | Oppositional Defiant Disorder (ODD) | Classic Autism Profile |
|---|---|---|---|
| Primary Motivation | Overwhelming anxiety and a need to maintain autonomy and control. | A need to challenge authority and engage in power struggles. | A need for predictability, routine, and sensory regulation. |
| Response to Demands | Avoids demands using social strategies (excuses, charm, distraction) or, if panicked, has a meltdown. | Directly refuses, argues, and is openly defiant toward authority figures. | Resists due to sensory distress, broken routines, or difficulty with transitions. |
| Social Interaction | Can appear socially savvy on the surface, but social understanding can be uneven. Uses social skills to avoid demands. | Often involves conflict and arguing with adults or peers. | May have challenges with social cues, reciprocity, and prefer solitary activities. |
| Flexibility | Appears to have "mood swings" or sudden changes; resists even enjoyable activities if they are presented as a demand. | Consistently oppositional, especially with authority figures. | Prefers sameness and routine; becomes distressed by unexpected changes. |
| Response to Praise | Can feel like a demand, leading to increased anxiety and avoidance of the praised behavior. | May be suspicious of praise or see it as a form of manipulation. | Typically responds positively to genuine praise and encouragement. |
This kind of comparison helps highlight the subtle but significant distinctions that a skilled evaluator is trained to recognize.
This infographic lays out some of the biggest challenges in the assessment process, which is why a nuanced, expert clinical approach is so essential.
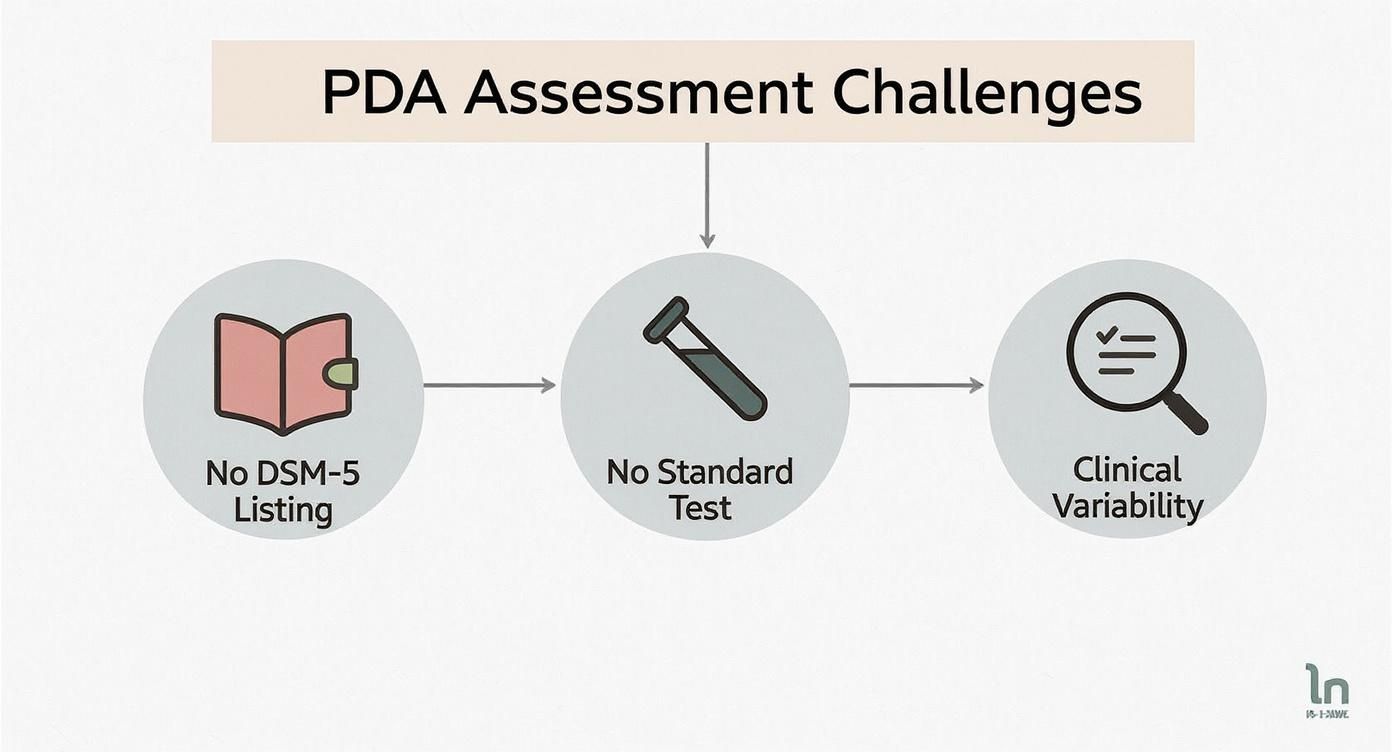
As you can see, without a standardized test or official diagnostic criteria to lean on, the clinician's expertise in recognizing these subtle patterns becomes the most important tool in the entire process.
The Comprehensive Assessment Process
To get the full picture, clinicians have to gather information from multiple sources. A detailed developmental history from parents is crucial for understanding when these patterns first started and how they've evolved. Reports from teachers and direct observation—whether in person or via telehealth—offer real-world examples of how the person navigates demands across different settings.
This 360-degree view helps the clinician spot the consistent patterns that point more strongly toward one profile over another. This ensures the final understanding is accurate and, most importantly, leads to support that is genuinely helpful.
When Is It Time to Seek a Professional Evaluation?
Knowing when to move from suspecting a Pathological Demand Avoidance (PDA) profile to seeking an official evaluation can feel like a tough call. It's often the point where the demand avoidance starts causing major disruptions in daily life—impacting school, family relationships, and the overall well-being of everyone involved.
If you're seeing a constant pattern of avoidance that leads to intense distress, school refusal, or makes it impossible to keep friends or a job, that’s a clear sign. These aren't just "behavior problems." They're flags for a deep, underlying anxiety that needs a very specific kind of support.
Another huge signal is when you've tried all the standard strategies for classic autism or ODD, and they just don't work. Or worse, they make things escalate. This is the moment many families realize they're dealing with something entirely different that requires a fresh, specialized perspective.
Your Roadmap to a Formal Assessment
The idea of pursuing an evaluation can feel overwhelming, but it’s much more manageable if you break it down into a few clear steps. The main goal is to find a professional who truly gets the nuances of the PDA profile and can provide an assessment that is both accurate and genuinely helpful.
Here’s a simple guide to get you started on the right path:
- Start a Conversation with Your Doctor: Your family doctor or pediatrician is a great first stop. They can help rule out any other medical concerns and give you a referral to a specialist, like a clinical psychologist or developmental pediatrician.
- Find a Specialist with Neurodiversity Experience: Look for clinicians who specifically mention that they have experience with the autism spectrum and its many different presentations. When you first reach out, don't hesitate to ask them directly if they're familiar with the PDA profile.
- Document Key Behaviors: Before your appointment, start keeping a simple log of specific examples of demand avoidance. Make a note of the demand, the reaction, and what happened next (e.g., distraction, making excuses, a meltdown). This kind of real-world information is priceless for a clinician.
- Gather a Detailed History: Pull together a timeline of your child's developmental milestones, their experiences in school, and how they've navigated social situations. The more complete the history you can provide, the clearer the picture will be for the assessment team.
Think of preparing for an evaluation as gathering evidence, not making a diagnosis yourself. Your job is to give the expert the detailed, real-world context they need to see the whole person and connect the dots.
Why Early Identification Matters So Much
Seeking an evaluation as early as you can is incredibly important, partly because the way PDA traits present can change over time. Research shows that while many autistic children show PDA traits, these features can often evolve or become less pronounced by the time they reach adulthood.
For example, a study in the Faroe Islands found that while 18% of autistic individuals met the criteria for a possible PDA diagnosis in childhood, only one out of nine still met the full criteria as they got older. This really highlights how identifying these traits early on can lead to better, more tailored support during those critical developmental years. You can read the full research on how PDA characteristics evolve to learn more about these changes. Ultimately, an early and accurate pathological demand avoidance test or evaluation gives you the best shot at putting strategies in place that really help.
Exploring Telehealth Options for a PDA Assessment

Finding a clinician with deep expertise in the Pathological Demand Avoidance (PDA) profile can feel like looking for a needle in a haystack. This is especially true if you don't live near a major city. Fortunately, telehealth has completely changed the game, making expert assessments more accessible than ever, no matter where you are.
For many people, especially those with PDA traits, the traditional in-person assessment is incredibly stressful. Just the demand of traveling to an unfamiliar clinic, navigating a new building, and meeting strangers can crank up anxiety. This can unintentionally mask the very behaviors a clinician needs to see.
The Advantages of a Remote Evaluation
A remote assessment lets the individual stay right in their own home—a familiar, low-demand space where they feel safe and comfortable. This setting often leads to a much more authentic and accurate observation of how they communicate and respond to everyday pressures.
The benefits here are huge:
- Reduces Travel Stress: You get to skip the logistical and emotional strain of getting to and from an office.
- Increases Comfort: Being in a familiar environment lowers that baseline anxiety, giving the clinician a clearer picture of your child's or your own profile.
- Wider Access to Specialists: Families are no longer limited by geography and can connect with leading experts in PDA from anywhere.
This approach is especially powerful for observing how a person navigates their daily life, offering insights that are almost impossible to capture in a sterile, clinical setting.
A telehealth assessment isn’t just a video call; it’s a window into an individual's world. It allows a clinician to observe interactions and behaviors in a natural context, which is essential for a nuanced and accurate evaluation of a PDA profile.
What a Comprehensive Telehealth Assessment Involves
Don't mistake "remote" for "less thorough." A high-quality remote pathological demand avoidance test or evaluation is just as comprehensive as an in-person one. Experienced professionals follow a structured, multi-faceted process to gather all the information they need. At the Sachs Center, we’ve refined our telehealth neuropsychological testing to ensure we get a complete and accurate diagnostic picture every time.
A typical remote assessment includes several key parts:
- In-Depth Caregiver Interviews: We hold detailed virtual conversations to gather a full developmental history and get a real understanding of current challenges.
- Virtual Observations: These are live, interactive sessions where we can observe the individual’s social communication style and how they respond to indirect demands.
- Collaboration with Support Systems: We gather input from teachers, therapists, and other professionals through secure video calls or by reviewing their reports.
When you're looking into remote options, make sure you choose a provider that takes security seriously. A critical piece of this is ensuring HIPAA-compliant data transfer to protect sensitive personal health information from start to finish.
By combining all these elements, a remote assessment offers a valid and robust pathway for families seeking specialized help, effectively breaking down the geographical barriers to expert care.
Common Questions About PDA Evaluation
When you're trying to make sense of a Pathological Demand Avoidance (PDA) profile, it's easy to feel overwhelmed with questions. Understanding the next steps can feel daunting, so let's walk through some of the most common queries we hear from families navigating this process.
What Is the Best Age to Seek a Diagnosis?
There’s no magic number here, but identifying a PDA profile earlier in life is almost always a huge help. When we can spot these traits in childhood, we can get the right kind of support in place at home and school during those critical developmental years. It can mean the difference between years of misunderstanding and an environment that actually works for them.
That said, it is never too late. We see many adults who are just now discovering the PDA profile, and for them, it’s a lightbulb moment. It finally explains a lifetime of anxiety, avoidance, and burnout. Getting an assessment as an adult can be incredibly validating, offering a new way to understand yourself and develop coping strategies that finally click.
What if I Can't Find a Clinician Who Recognizes PDA?
This is a real and frustrating hurdle for many families, especially since PDA isn't an official diagnosis in the DSM-5 yet. If you’re struggling to find a local expert who’s well-versed in PDA, the best approach is to seek out a clinical psychologist or neuropsychologist who specializes in complex presentations of autism and neurodiversity.
When you reach out, you don’t even have to use the "PDA" label. Just describe what you're seeing in plain terms.
Talk about the core features you’re noticing. You could explain that you’re seeing an extreme, anxiety-driven avoidance of everyday demands, that social strategies are being used to maintain a sense of control, and that all the typical behavioral approaches have backfired.
This kind of description gives an experienced clinician the essential clues they need. They can then conduct a thorough pathological demand avoidance test and evaluation, even if they don't use the specific term "PDA" in their final report.
How Does a PDA Profile Change Support Strategies?
This is the most critical piece of the puzzle. Identifying a PDA profile completely flips the script on traditional support. Many autistic individuals find comfort in structure, clear rules, and direct instructions. But for someone with a PDA profile, those very things can feel like a threat and trigger a fight-or-flight response.
- Traditional Autism Support: This often leans on predictability, direct communication, and clear rules to lower anxiety. Rewards and praise are common tools.
- PDA-Informed Support: This approach is all about lowering demands, offering choices, communicating indirectly, and working collaboratively. The goal is to build emotional safety and autonomy, not enforce compliance.
For instance, instead of saying, "It's time for homework," a PDA-friendly approach sounds more like, "I wonder how we could get that science project started later?" It’s a subtle shift, but it removes the direct demand and defuses the anxiety, making cooperation much more likely. Grasping this difference is the key to finding strategies that genuinely help.
At the Sachs Center, our telehealth evaluations are led by specialists who deeply understand the nuances of PDA and other complex neurodivergent profiles. We're here to provide the clarity you need to move forward with confidence and the right kind of support. Learn more about our virtual assessment process and book an appointment today.